Week 13 — Categorical outcomes
MATH 21003 · Introduction to Statistical Methods · Fall 2026 · Week 13 (Nov 16–20, 2026)
Why this week matters
For two weeks we have asked the questions of inference about a single number — is this one proportion different from a benchmark? is this one mean what we expected? This week the question becomes a comparison: two groups, a yes/no outcome, and the everyday question that runs through medicine, public health, and the life sciences — does the rate differ between these groups, and by how much? A treated group versus a control group. People who took a drug versus people who did not. Exposed versus unexposed.
The honest answer needs two layers. First, how big is the difference? We have three standard ways to size it up — the risk difference, the relative risk, and the odds ratio — and they are not interchangeable. Second, could the difference be chance? That is the same hypothesis-testing engine from Week 12, now pointed at a two-way table through the chi-square idea. The rhythm: Monday builds the three risk measures from a 2×2 table; Wednesday turns the table into a test — expected counts and the chi-square logic; Friday reads a real clinical categorical-outcome case and writes a careful conclusion. The recurring caution this week: a number that compares two groups can be right and still be misread — a large relative risk on a rare outcome can be a tiny absolute change, and “associated” is still not “caused.”
A bridge from Weeks 10 and 12
You have already done most of the hard thinking. Back in Week 10 you read two-way tables for diagnostic testing, you worked with risk as a conditional probability — the chance of an outcome given a group — and you learned the base-rate caution that a rare condition makes a positive result harder to interpret. Everything this week is built on that table-reading. Relative risk and the odds ratio are just two of those conditional probabilities (or odds) placed side by side as a ratio.
And from Week 12 you already own the inference engine: a test statistic, a p-value, and a significance level, with the p-value read as strength of evidence (the habit from Week 11). This week adds no new logic of testing — it applies the Week 12 engine to a categorical comparison. When you read a chi-square result on Wednesday, you are doing exactly what you did with a \(t\)- or \(z\)-test: ask whether what you see is more than chance would produce.
Monday: rates, risks, and three ways to compare two groups
Start with the object everything rests on — the 2×2 table. Two groups down the side, a yes/no outcome across the top, four counts inside. Label them \(a\), \(b\), \(c\), \(d\):
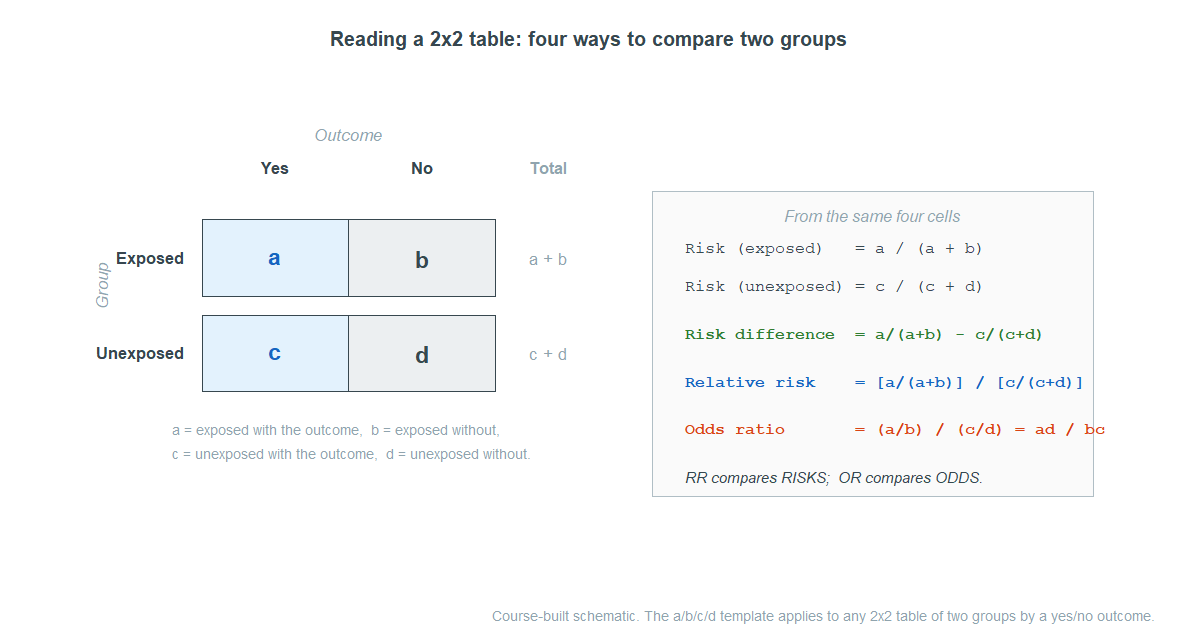
The risk of the outcome in a group is just its proportion: for the exposed group, \(a/(a+b)\). From the two risks you can build three comparisons, each answering a slightly different question.
Risk difference — how many more cases per 100? Subtract the two risks. In the opportunity-cost-style clinical world a clean example is the CPR study you met last week: survival was \(11/50 = 0.22\) in the control group and \(14/40 = 0.35\) in the treatment group, a risk difference of
\[0.35 - 0.22 = 0.13,\]
13 more survivors per 100 patients. The risk difference is an absolute measure, on the same scale as the risks themselves, and it travels with a confidence interval just like Week 12: the \(90\%\) interval here is \((-0.027,\ 0.287)\). Because that interval contains \(0\), “no difference” is still plausible — the study cannot rule out chance. Contrast the fish-oil trial, where the heart-attack rate was \(0.0112\) on fish oil versus \(0.0155\) on placebo, a risk difference of \(-0.0043\) with a \(95\%\) interval of \((-0.0071,\ -0.0015)\). That interval lies entirely below \(0\), so fish oil really did lower the rate — by about \(0.15\) to \(0.71\) percentage points. Small, but real.
Relative risk — how many times as likely? Divide the two risks instead of subtracting. A relative risk (RR) of \(2\) means the outcome is twice as likely in one group as the other; an RR of \(0.73\) means the exposed group has \(73\%\) of the risk — a reduction. Relative risk is a ratio, which makes it feel dramatic, and that is exactly its trap: a relative risk can be large while the absolute change is tiny. “Doubles your risk” sounds alarming, but doubling a \(1\)-in-a-million risk is still almost nothing. Always read a relative risk next to the underlying risks.
Odds ratio — how do the odds compare? Odds are not the same as probability: the odds of an outcome are (cases)/(non-cases), so \(a/b\) in the exposed group. The odds ratio (OR) divides the two groups’ odds, and it has a tidy shortcut straight from the table:
\[\text{OR} = \frac{a/b}{c/d} = \frac{ad}{bc}.\]
An odds ratio of \(1\) means no association; above \(1\) the exposure goes with higher odds of the outcome; below \(1\), lower. The odds ratio matters because of how some studies are built. In a case-control study, researchers start by collecting people who already have the outcome (the cases) and people who do not (the controls), then look backward at exposure. That design is the only practical way to study a rare disease — but it means you cannot read the true risk of the disease from the table, because the researchers chose how many cases to include. You can still compute the odds ratio, and that is why case-control studies report it.
A clean clinical example: a case-control study of newborn pulmonary hypertension (PPHN) and a class of antidepressants (SSRIs) sampled \(337\) infants with PPHN and \(836\) without, then checked SSRI exposure. Among the cases, \(14\) were exposed and \(323\) were not; among the controls, \(6\) were exposed and \(830\) were not. The odds ratio is
\[\text{OR} = \frac{14 \times 830}{323 \times 6} = 6.00.\]
The odds of SSRI exposure were six times higher for infants with PPHN than for those without — strong evidence of an association worth investigating. Notice what we did not say: we did not say PPHN is “six times as likely,” because in a case-control design we cannot estimate that risk at all.
(One bridge to keep straight: odds ratios also show up in logistic regression — the Week 9 model for yes/no outcomes — but this week we read them directly from a 2×2 table, no model required.)
When relative risk and the odds ratio disagree
Students often treat RR and OR as the same number. They are not, and the gap between them depends on how common the outcome is.
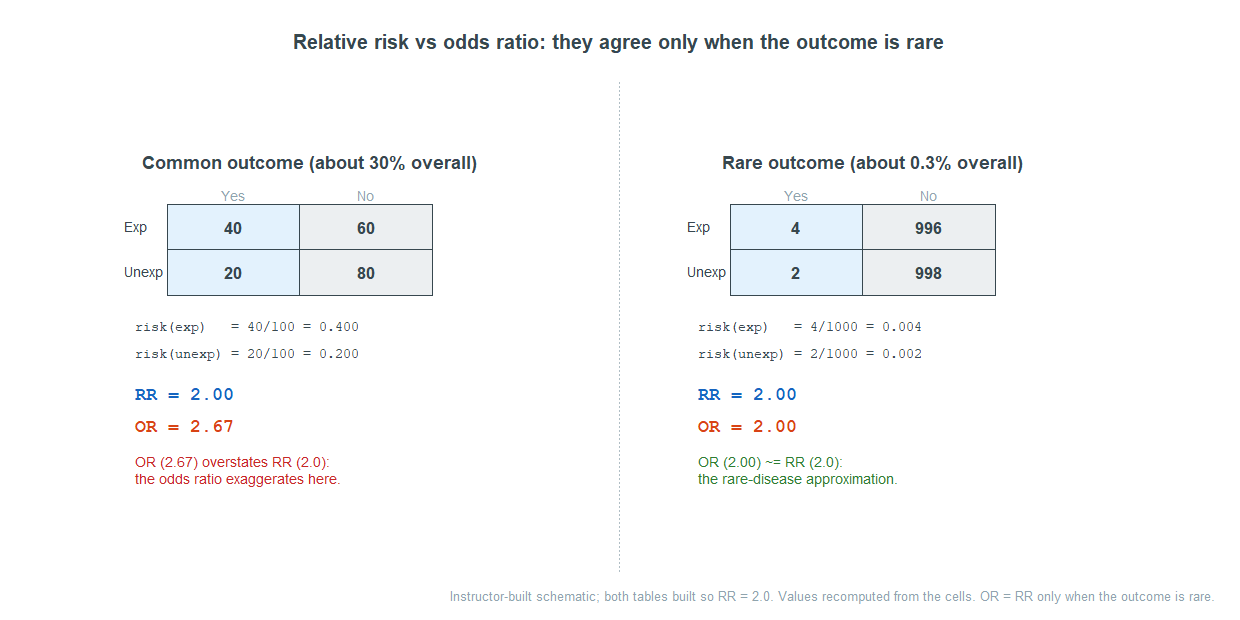
Both tables are rigged to have the same relative risk of \(2.0\). When the outcome is common (about \(30\%\) here), the odds ratio inflates to \(2.67\) — it overstates the relative risk. When the outcome is rare (about \(0.3\%\)), the odds ratio is \(2.00\), essentially equal to the relative risk. This is the rare-disease approximation: an odds ratio is a good stand-in for a relative risk only when the outcome is uncommon. It is why headlines that quote an odds ratio for a common outcome as if it were a relative risk can badly mislead.
Wednesday: two-way tables, expected counts, and the chi-square idea
Sizing up the difference is half the job. The other half is the Week 12 question: could the pattern in this table be chance? For categorical data the tool is the chi-square test of independence, and its logic is simpler than its name.
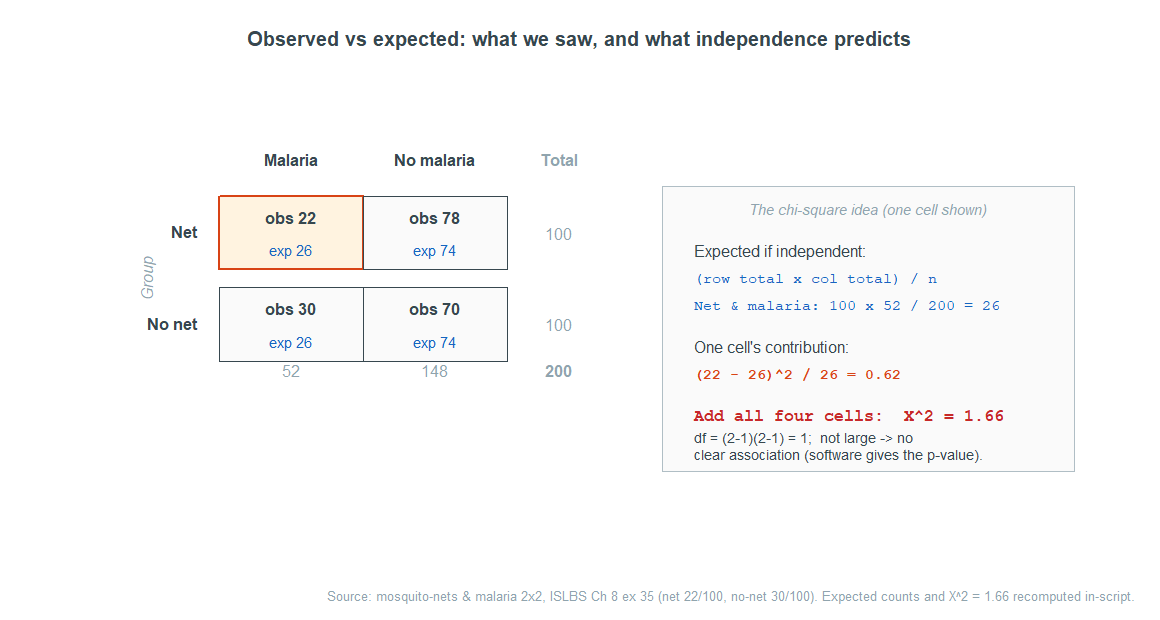
Begin with a question: what would the table look like if the two variables were unrelated? If a group made no difference, each group should show the same outcome rate as the table overall. Those “if-independent” counts are the expected counts, and they come from a single rule:
\[\text{expected count} = \frac{(\text{row total}) \times (\text{column total})}{\text{table total}}.\]
You do not memorize a derivation; you read the expected count as what we would expect in this cell if the two variables were independent. Then you compare the observed counts to those expected counts. Where the table departs from independence, observed and expected pull apart; where they match, the table looks independent.
The chi-square statistic adds up, over every cell, how far observed sits from expected — squared, then scaled by the expected count:
\[\chi^2 = \sum \frac{(\text{observed} - \text{expected})^2}{\text{expected}}.\]
You will not crank a full chi-square by hand in this course; the point is the logic the formula encodes. Bigger gaps between observed and expected counts make a bigger \(\chi^2\), and a bigger \(\chi^2\) means a smaller p-value — stronger evidence the variables are related. The p-value itself is a right-tail area, read off a chi-square curve whose shape is set by the degrees of freedom, \(df = (\text{rows} - 1)\times (\text{columns} - 1)\).
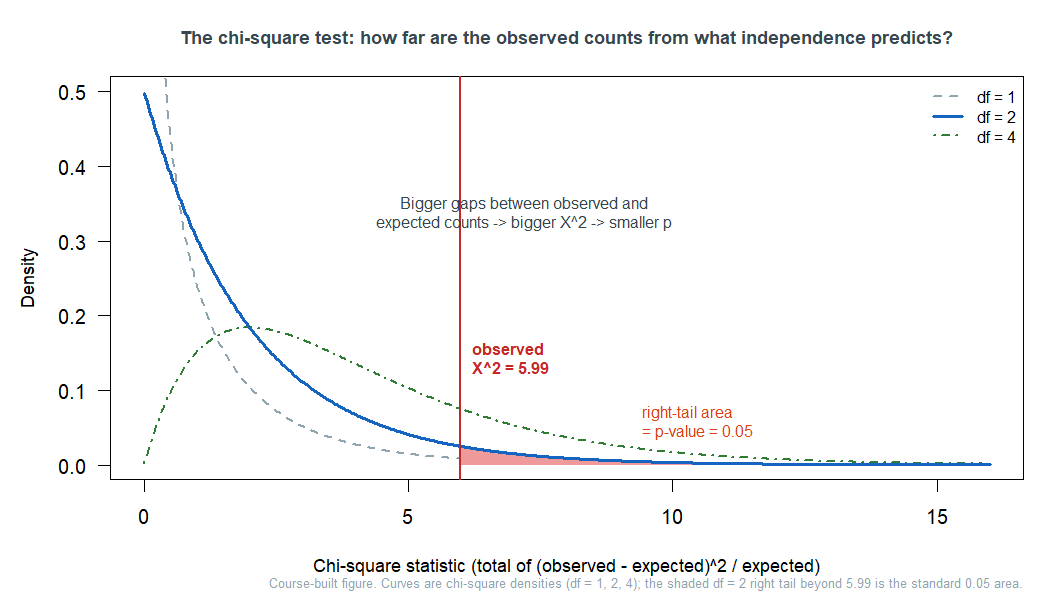
So the whole test reads as one sentence: the chi-square measures how far the observed counts stray from what independence predicts, and the p-value is the chance of straying that far if the variables were truly unrelated.
Two contrasting reads make it concrete. In the mosquito-net table above, \(\chi^2 = 1.66\) on \(1\) degree of freedom — a small statistic, no clear association in these \(200\) children, even though the observed risks (\(0.22\) with a net versus \(0.30\) without) hint at a benefit. The hint is real but the evidence is thin: a point estimate is not proof, and a small study can leave chance on the table. Compare a study of how an iPod-selling script affected whether sellers disclosed a known defect: there the observed and expected counts pulled far apart, giving \(\chi^2 = 40.13\) on \(2\) degrees of freedom — astronomically far into the tail, decisive evidence the script and the disclosure were related.
Comparing two proportions, formally
When the table is exactly 2×2, the chi-square test and the two-proportion \(z\)-test are two routes to the same conclusion, and the \(z\) route fits last week’s machinery exactly. The test statistic keeps the familiar form,
\[z = \frac{(\hat p_1 - \hat p_2) - 0}{\text{SE}},\]
— an estimate, minus the null value of “no difference,” over a standard error — and the p-value is a tail of the normal curve. Take the mammogram study: over \(\approx 90{,}000\) women, breast-cancer deaths were \(500\) of \(44{,}925\) in the screened group and \(505\) of \(44{,}910\) in the control group. The difference in death rates is about \(-0.00012\), giving \(z = -0.17\) and a two-sided p-value of \(0.8650\) — nowhere near significant, so we fail to reject: no detectable difference in breast-cancer deaths. The chi-square test on the same \(2\times2\) table agrees, with \(\chi^2 = 0.02\) on \(1\) degree of freedom (for a \(2\times2\) table the two tests are equivalent, so use whichever the output shows).
The mammogram study also makes a Week-12 point vivid: with a sample this enormous, the test had ample power to detect even a small effect — and it found none. That is the honest opposite of the other classic warning: huge samples can make a trivial difference “significant” — and, just as usefully, they can give us enough precision to rule out any difference large enough to matter in context. A failure to reject is never proof of “no effect”; what a very large, precise study can support is that any remaining difference is small enough to be practically unimportant. Statistical discernibility and practical importance are still two different things.
Friday: reading a clinical categorical-outcome case
Friday pulls the week together on a real case, read end to end. The skill is not computing — it is interpreting: given a 2×2 table or a printed chi-square result, say what the comparison is, choose the right measure, and write a conclusion a careful reader would trust.
Work the mosquito-net case as that exercise. The risk of malaria was \(22/100 = 0.22\) with a net and \(30/100 = 0.30\) without — a risk difference of \(-0.08\) and a relative risk of \(0.22/0.30 \approx 0.73\), meaning netted children had about three-quarters the risk. On its face, a protective effect. But the chi-square is only \(1.66\) on \(1\) degree of freedom — the evidence from these \(200\) children is not strong enough to rule out chance. The responsible conclusion holds both thoughts at once: the observed pattern suggests nets help, but this study is too small to be convincing; a larger trial is needed. That sentence — an effect estimate and an honest read of the evidence behind it — is exactly what Week 13 is training.
A second discipline carries over from all term: a chi-square test, or a risk ratio, shows association, not causation by itself. Whether you can say “caused” still depends on the study design from Weeks 2 and 6 — a randomized experiment earns causal language; an observational comparison does not, no matter how small the p-value.
Common mistakes
- Reading an odds ratio as a probability or a relative risk. An OR of \(6\) does not mean “six times as likely.” It compares odds, and it only approximates a relative risk when the outcome is rare.
- Quoting a relative risk without the absolute risk. “Doubles the risk” can mean a huge change or a negligible one. Always pair RR with the underlying risks or the risk difference.
- Trying to get a risk or a relative risk from a case-control study. The design fixes how many cases there are, so the disease risk is not estimable — report the odds ratio.
- Thinking expected counts are something you observed. Expected counts are what independence would predict, not data. The test compares the two.
- Treating a big \(\chi^2\) as proof of a strong or important effect. A large \(\chi^2\) (or tiny p) rules out chance; it says nothing about the size of the association, and with huge samples even trivial associations clear the bar.
- Saying “associated” and meaning “caused.” Chi-square and risk ratios measure association. Causation still rides on the study design.
What you should be able to do by Friday
By the end of Week 13 you should be able to:
- read a 2×2 table and compute a risk, a risk difference, a relative risk, and an odds ratio (\(ad/bc\)), and say in words what each one means;
- explain why a case-control study reports an odds ratio rather than a risk, and when an odds ratio approximates a relative risk;
- explain expected counts as “what we would expect if the variables were independent,” and read the chi-square logic — bigger observed-versus-expected gaps give a bigger \(\chi^2\) and a smaller p-value;
- read a chi-square result (the statistic, the degrees of freedom, the p-value) or a two-proportion test and conclude in context;
- keep association separate from causation, and a relative measure separate from an absolute one;
- write a careful conclusion that pairs an effect estimate with an honest read of the evidence behind it.
Assignments this week
- Monday check. A short in-class concept check on reading a 2×2 table: compute a risk, a risk difference, and a relative risk, and say what each means. Plan for about 3–5 minutes. Sheet: Week 13 Monday exit ticket.
- Wednesday check. A short application on a risk/odds table: from a 2×2, find the relative risk and the odds ratio, or read a chi-square result and state the conclusion. Plan for about 8–12 minutes. Sheet: Week 13 Wednesday exit ticket.
- 🔒 Friday quiz — handled through Blackboard or in class as directed. The quiz prompt is not posted here. Timing and submission details live in Blackboard.
- 🔒 Project checkpoint — this week falls in the course project window. Your checkpoint deliverable and its due date are posted in Blackboard, not here.
- No new homework opens this week. Homework 6 (Weeks 11–12) was the last biweekly set; from here the project carries the synthesis work.
Read more in IMS / ISLBS
The course page above is the main explanation for this week. For a second voice at similar depth:
- IMS — Introduction to Modern Statistics, Chapter 17 Inference for comparing two proportions (the risk difference, the two-proportion \(z\) confidence interval and test, with the CPR, fish-oil, and mammogram examples) and Chapter 18 Inference for two-way tables (expected counts, the chi-square statistic and distribution, degrees of freedom, and reading the p-value, with the iPod study). Read the worked examples and output; skip the by-hand derivations and the randomization/bootstrap passes — those simulation methods belong to Week 11, and here we read classical results. Note that IMS Chapter 17 covers the risk difference but not relative risk or the odds ratio.
OpenIntro book page: https://www.openintro.org/book/ims/ - ISLBS — Introductory Statistics for the Life and Biomedical Sciences, Chapter 8 Inference for categorical data is the clinical and risk-measure source for this week. It is where relative risk and the odds ratio are developed — §8.5 on outcome-based (case-control) studies is the source for the odds ratio, the \(ad/bc\) shortcut, the rare-disease approximation, and the PPHN/SSRI example — and §8.2–§8.3 give the clinical two-proportion and chi-square framing (mammogram, and the mosquito-net and related two-way tables). You can skip the sample-size formulas (§8.1.3) and the exact-test hand computations, which are beyond this course.
OpenIntro book page: https://www.openintro.org/book/biostat/
Looking ahead: Week 14 turns from a single comparison to many of them at once — how separate studies are combined into one estimate through meta-analysis and forest plots. The risk ratios and odds ratios you read this week are exactly the quantities a meta-analysis pools. That is next week’s business.
Sources adapted in this lesson: This page draws on OpenIntro Introduction to Modern Statistics (2e), Çetinkaya-Rundel & Hardin: Chapter 17 for the difference in proportions, the two-proportion \(z\) confidence interval and test, and the CPR, fish-oil, and mammogram examples; and Chapter 18 for two-way tables, expected counts, the chi-square statistic and distribution, degrees of freedom, and the iPod example. It draws on OpenIntro Introductory Statistics for the Life and Biomedical Sciences, Vu & Harrington, Chapter 8 — the clinical and risk-measure source — for relative risk and the odds ratio (§8.5, case-control studies, including the PPHN/SSRI example and the \(ad/bc\) shortcut) and for the clinical two-proportion and chi-square framing (§8.2–§8.3, including the mammogram and mosquito-net tables). Relative risk and the odds ratio are taken from ISLBS; IMS Chapter 17 supports the risk difference and two-proportion inference but does not supply RR or OR. OpenIntro materials are CC BY-SA 3.0. Source files: IMS and OI-Biostat. The public figures are course-built schematics or reconstructions using the source-grounded values documented in the Week 13 extraction notes; the two-way-table template and the relative-risk-versus-odds-ratio comparison are labeled instructor-built schematics, and the mosquito-net chi-square figure recomputes its expected counts and statistic (\(\chi^2 = 1.66\)) from the displayed counts.